OCaPE: Pharm #1 -
OCaPE: Pharm #1 -
Blood Pressure
Hypertension (1)
Give an idiopathic cause of hypertension, and a secondary cause of hypertension?
Idiopathic: genetic, overweight, alcohol, salt intake, sedentary lifestyle
Secondary: coarctation of the aorta, renovascular, renal parenchymal,
Conn’s, phaeochromocytoma, Cushing’s, drugs (2)
Write out the equation for calculating blood pressure.
Explain the definition of each component of the equation.
BP = CO x TPR
Cardiac output: volume of blood pumped out of the left ventricle
Total Peripheral Resistance: amount of force exerted on circulating blood by
vasculature of the body (3)
What is the initial most appropriate course of action?
Repeat blood pressure (as it may be raised due to White Coat Hypertension)
(1)
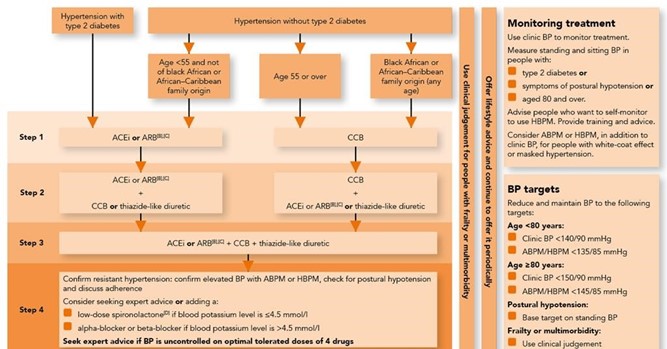
After discussion with a senior doctor, you have decided to start him on medication. What two classes of drugs can you start off with?
Give one example for each.
ACE inhibitors: ramipril, lisinopril, perindopril, enalapril
Angiotensin II Receptor Blockers: losartan, Irbesartan, valsartan, candesartan (4)
Draw a flow chart to demonstrate the mechanism of action for both drugs.
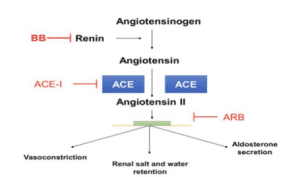 (2)
(2)The patient returns 3 months later, and his hypertension has not improved.
Give the name of a drug you can prescribe him next.
Beta Blockers: Bisoprolol, atenolol, propranolol, carvedilol (1)
The patient’s daughter has a similar condition but is pregnant. Which drug can be prescribed for her?
Labetalol (think Labour) (1)
Over the next year, the patient’s hypertension has not improved. The doctor suspects heart failure.
Why should verapamil not be prescribed?
Verapamil is a non- dihydropyridine Calcium Channel Blocker
Acts on both cardiac and peripheral tissue
Drug would lead to heart failure as it is negatively inotropic (decreases force
of contraction)
(3)
What calcium channel blocker should the doctors prescribe instead?
Describe the mechanism of action.
Dihydropyridine CCB: amlodipine, nifedipine, felodipine
Prevents Calcium from entering arterial smooth muscle, thus preventing
vasoconstriction.
Vasodilation occurs, reducing TPR, so BP falls,
(2)