OCaPE: ESR #2
OCaPE: ESR #2
Low Cortisol
You are a second year medical student at an endocrine clinic. A patient presents:
History: HIV positive female
Presentation: feels constantly tired and weak, thirsty all the time, low mood and loss of appetite. Persistent weight loss. Persistent cough, fever and night sweats. Started feeling faint and dizzy recently and noticed changes in her physical appearance

Hyperpigmented skin, hypotensive, polydipsia weight loss, persistent cough, fever and night sweats. (3)
What two follow-up investigations would you like to perform?
- adrenal CT, or CRH challenge (cortisol fails to increase, low aldosterone),
- blood tests (hyponatraemia, hyperkalaemia, high renin to aldosterone ratio) (3)
The doctors perform this test. Explain what these results are showing?
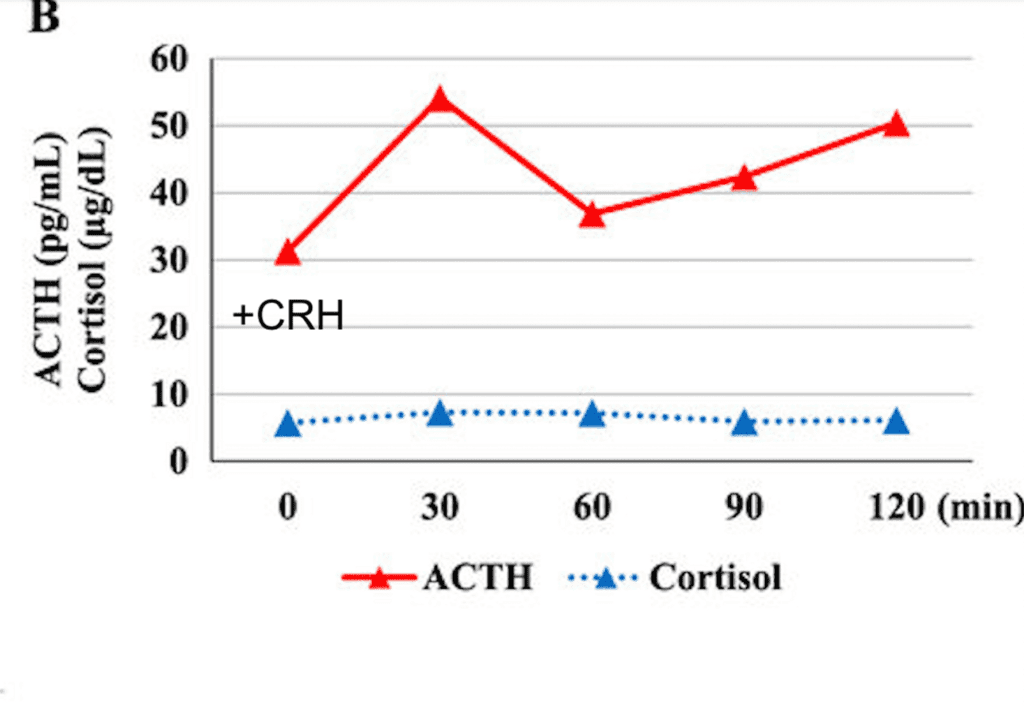
- CRH challenge
- Patient is given CRH
- Levels of ACTH increase as expected
- However, levels of cortisol do not increase (3)
Here are the blood results of the same patient.
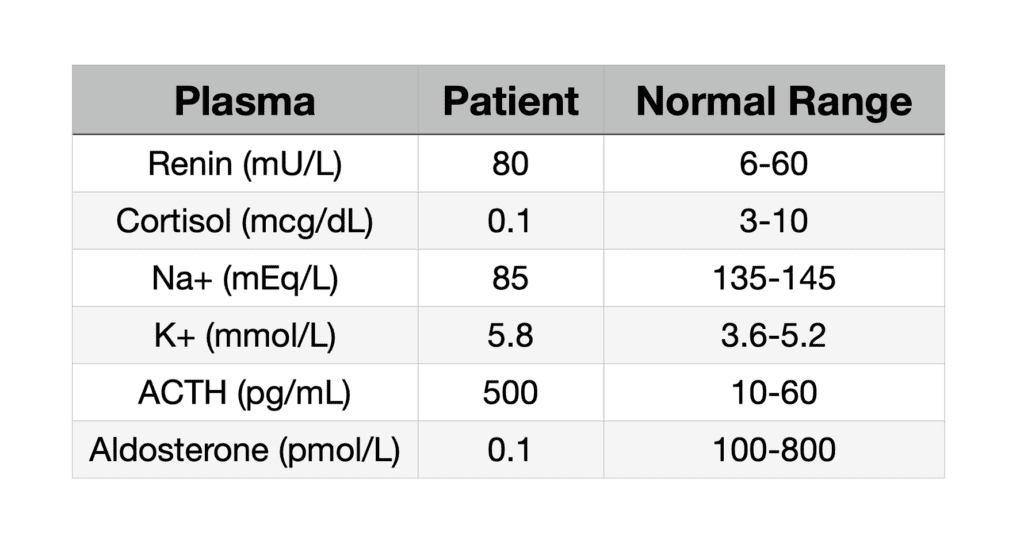
How does these and the CRH challenge explain the patient’s symptoms?
- Low cortisol (hypoglaecaemia)
- Low aldosterone (hypotension due to low plasma volume and therefore polydipsia)
- High levels of ACTH (loss of negative feedback)
- hyperkalaemia and hyponatraemia (reduced ENaC translocation),
- Addison’s disease
(5 – if Addison’s not mentioned max 3 marks)
Why does this condition cause hyperpigmentation?
Increased levels of ACTH by negative feedback (corticosteroid deficency)
Therefore increase in the precursors, POMC.
POMC is cleaved to ACTH and alpha-MSH
Increase in alpha-MSH is responsible for hyperpigmentation. (4)
What are the causes of this condition?
Autoimmune destruction of the adrenal cortex
following tuberculosis or HIV infection
or sudden withdrawal of steroid medication.
(2)
What treatment is given for people with this condition?
Lifelong glucocorticoids (hydrocortisone) and mineralocorticoids
must wear steroid dependent bracelet
to get urgent treatment for an adrenal crisis (3)