so less dopamine is produced for the basal ganglia

💊L-DOPA- synthetic dopamine
💊Ropinirole– D2 receptor agonist
💊Apomorphine– D1 and D2 receptor agonist
💊Amantadine– blocks dopamine reuptake channel
💊Domperidone– D2 antagonist (stops nausea and vomiting by preventing dopamine activating the chemoreceptor trigger zone.
💊 Selegiline + Entacopone– drugs that allow dopamine to remain
in high quantities in the CNS, without being further
converted to other products
💊Carbidopa– dopa-decarboxylase inhibitor (prevents
dopamine leaving the CNS to the PNS)
 Benzodiazepines (“-lam/-pam”)
Benzodiazepines (“-lam/-pam”)
- GABAa agonists. open Cl- channels more frequently for more hyperpolarisation.
(bind at the alpha-gamma junction on the GABA channel) - Good for sedative, muscle relaxant, amnesia (surgeries)
4 Hours: Midazolam
15 Hours: lorazepam, oxazepam, temazepam
24 Hours: alprazolam, nitrazepam
48 Hours: chlordiazepoxide (lithium) diazepam (valium)
60 Hours: clonazepam, flurazepam Side Effects: confusion, drowsiness, tolerance, dependence (tremor), respiratory depression
 with alcohol
with alcohol
(Flumazenil- used in BDZ overdose)
Buspirone- for general anxiety. (5HT agonist)
Barbiturates:
cause respiratory depression
- thiopental- anaesthetic
- phenobarbitone- epilepsy
Sleep:
antihistamines (H1), nytol, valerenic acid (valarion extract)
chlormethiazole- for elderly as no hang-over effect
Insomnia: transient -> intermediate -> chronic
 Z-drugs: (zzzz for sleep)
Z-drugs: (zzzz for sleep)
Zolpidem, zopiclone (REM deficiency)
Local anaesthetics (“-caine”) work by blocking Na+ channels to stop pain action potentials
Amide Types:
- (‘i’ before the “-caine”)
- Lidocaine, Prilocaine
- metabolised in liver
Ester Types:
- (no ‘i’ before the “-caine”)
- procaine, tetracaine
- metabolised in blood
General Anaesthetics (“-caine”) (drug induced reversible loss of consciousness)
Inhaled- (maintain anaesthetic):
- isoflurane, desflurane – GABA
- nitrous oxide, xenon, ketamine
- block NMDA (non-competitive), so Ca2+ cannot carry the pain signals to the post-synaptic neurone
- thiopentone, propofol, etomidate
- keep GABAa open for hyperpolarisation of post-synaptic neuron
Tetrabenazine- dopamine depletion (inhibit nigrostriatal pathway)
Restless leg – ropinirole (D2 agonist – desensitise to movement)
Tourettes – haloperidol (D2 antagonist)
Muscarinic Agonist
Pilocarpine (used in glaucoma – increases trabecular outflow)
Muscarinic Antagonist
atropine tropicamide
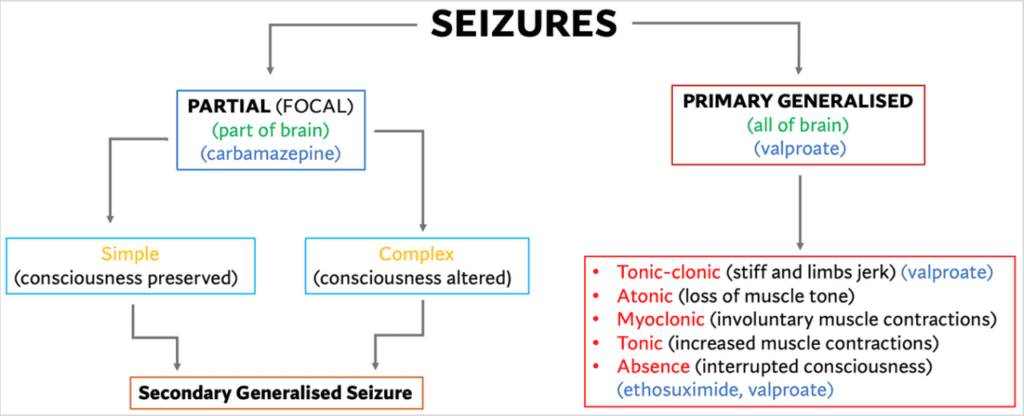
Na+ channel blockers: carbamazepine, phenytoin, valproate, lamotrigine Ca2+ channel blockers: ethosuximide, gapapentine GABA breakdown inhibitors: valproate, vigabatrin (keeps GABA working to hyperpolarise cells) GABAa modulator: benzodiazepines NMDA antagonist: felbamate AMPA antagonist: perampanel Vesicle depletion: levetiracetam (reduce glutamate release) GABA reuptake blocks: tiagabine (also used for anxiety)
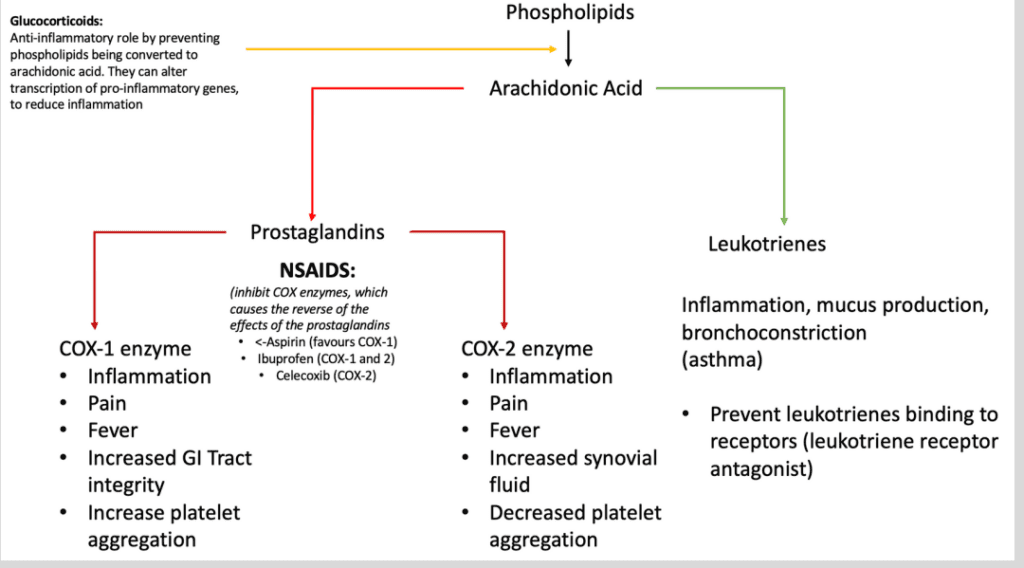
 Inflammatory pain
Inflammatory pain
NSAIDS
- Aspirin (COX-1 inhibitor)
- ibuprofen (COX-1 inhibitor)
- diclofenac (COX-2 inhibitor)
Steroids (SAIDS)
- hydrocortisol, cortisone
- (block conversion of phospholipids to arachidonic acid)
Triptans
- sumatriptan (‘-triptan” used for headaches and migraine
- inhibit 5HT receptors vasodilation
 Neuropathic Pain
Neuropathic Pain
- Na+ channel blockers- carbamazepine
- Ca2+ channel blockers- gabapentin, pregabalin
- NMDA blockers-
- ketamine (extreme pain)
- antidepressants
Opiates
- Mu, delta, kappa receptors.
- Mu- opiates
- Mu receptors- morphine, codeine, fentanyl (mimics endorphin,
opens K+ channels, hyperpolarising the post-synaptic neurone,
so pain signal cannot continue)
- Mu receptors- morphine, codeine, fentanyl (mimics endorphin,
- Mu- opiates
- delta- enkephalins
- kappa- dynorphin
💊 naloxone- opiate antagonist (give for overdose)
Others:
Paracetamol. (in overdose, treat with activated charcoal in first
hour, then use acetylcysteine) (can lead to hepatotoxicity)